 vi
vi 20-Sep-2025
20-Sep-2025
Introduction
In recent years, Phakic ICL (Implantable Collamer Lens) surgery has become a leading solution for correcting refractive errors in patients with severe myopia, hyperopia, and astigmatism. However, many patients still wonder: “Does Phakic ICL surgery cause regression or myopia recurrence?”
To answer this question, we need to understand the mechanism of the ICL lens, clinical effectiveness, and the factors that may influence long-term results.
What is Phakic ICL Surgery?
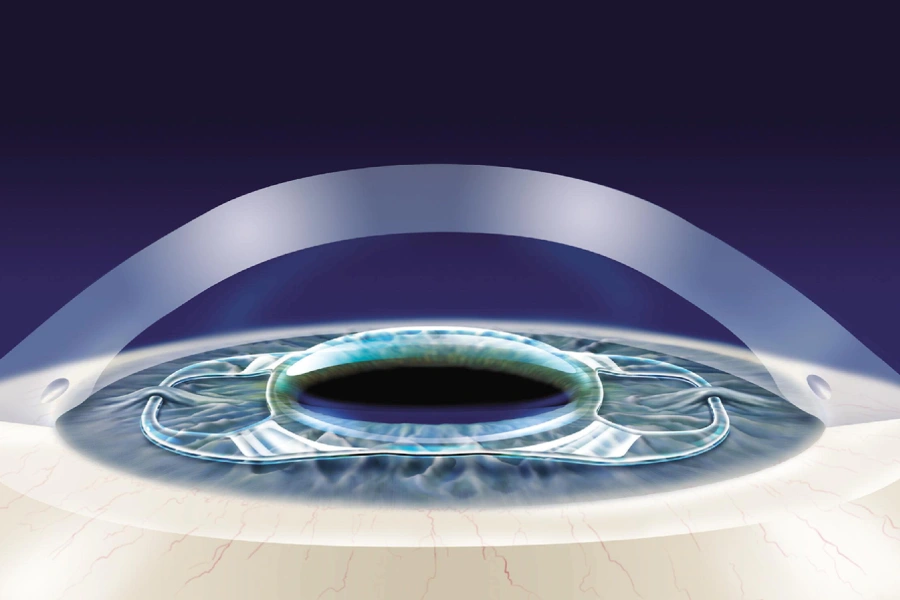
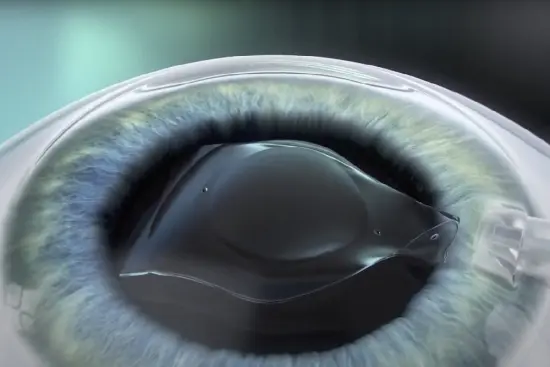
Phakic ICL lens in the eye
1. Overview of the Phakic ICL Method
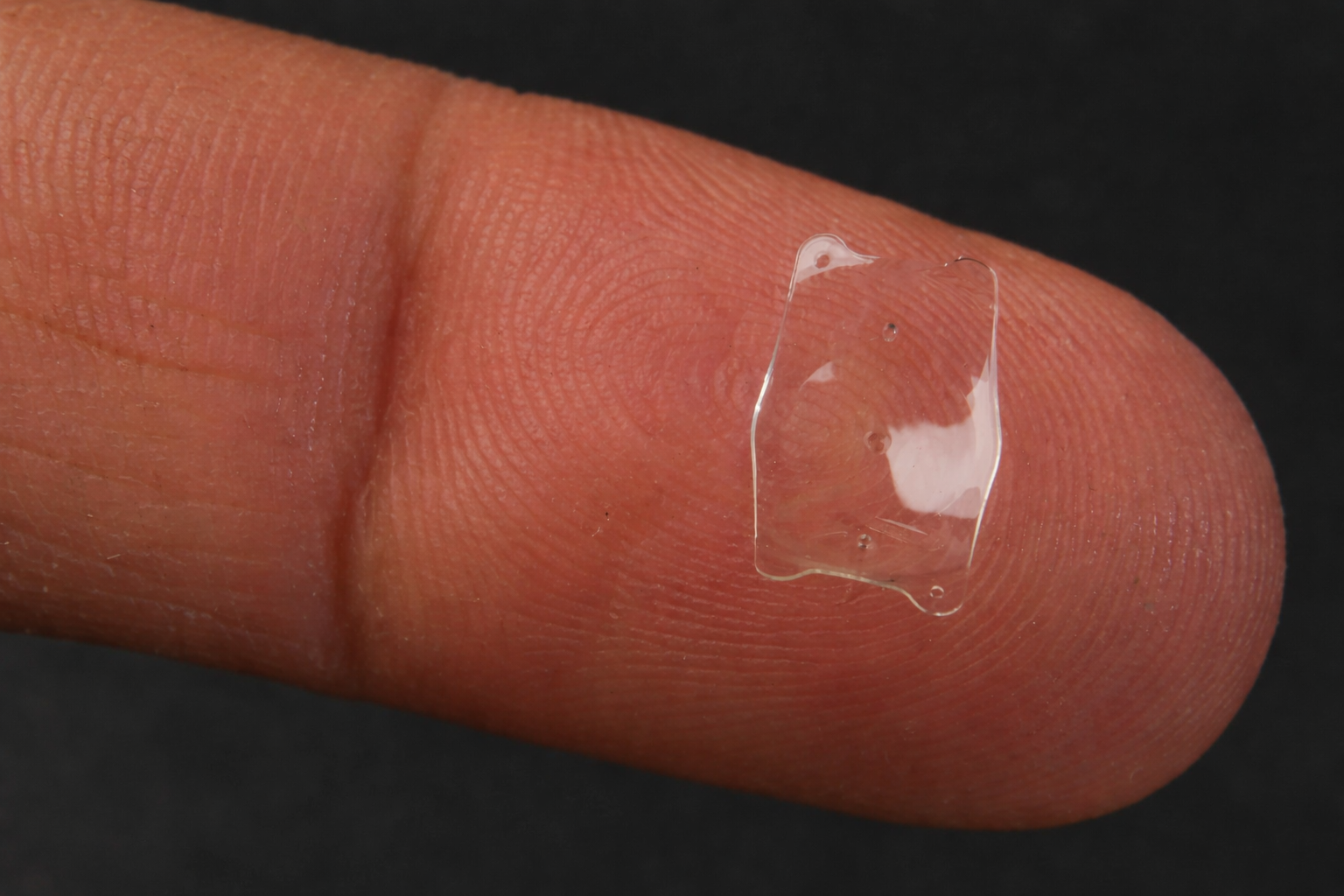
Phakic ICL (Implantable Collamer Lens) is a surgical technique where a specialized biocompatible lens is implanted inside the eye to correct refractive errors. The lens is made of Collamer® – a combination of collagen and polymer with high durability and biocompatibility, allowing the ICL lens to remain safely inside the eye for a lifetime.
The mechanism of Phakic ICL works similarly to wearing glasses, but instead of being placed outside, the ICL lens is positioned behind the iris and in front of the natural crystalline lens. This enables light to focus precisely on the retina, producing sharp vision without the need for glasses or contact lenses.
2. The Phakic ICL Surgery Procedure
Phakic ICL surgery is quick (10–20 minutes), painless, and allows fast recovery. The procedure typically includes:
- Step 1: Sterilization and eye stabilization.
- Step 2: Topical anesthesia with eye drops to ensure no pain during the procedure.
- Step 3: Creating a tiny incision (2–3 mm) at the corneal margin.
- Step 4: Inserting the folded ICL lens, which unfolds into the correct position inside the eye.
- Step 5: Final inspection and adjustment, with no sutures required as the incision self-seals.
Most patients rest for a few hours in the clinic and can resume light activities the following day.
How Phakic ICL Works
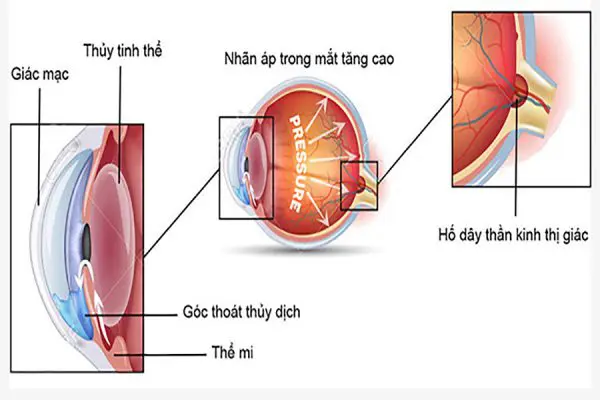
Diagram illustrating how Phakic ICL works
Unlike laser surgeries (LASIK, PRK, SMILE), which reshape or ablate corneal tissue, Phakic ICL does not alter the cornea. The implanted ICL lens functions like a microscopic converging lens, focusing light precisely on the retina.
This approach preserves the natural corneal structure, minimizes the risk of dry eye complications, and is suitable for patients with thin corneas or high myopia.
Causes of Regression After Refractive Surgery
With laser-based procedures, myopia regression can occur due to:
- Excessive corneal thinning, leading to weakness or ectasia.
- Unstable prescription prior to surgery (rapid progression in young patients).
- Residual myopia when the correction exceeds the safe ablation limit.
- Poor visual habits: prolonged screen time, reading in dim light, or lack of rest.
Does Phakic ICL Surgery Cause Regression?
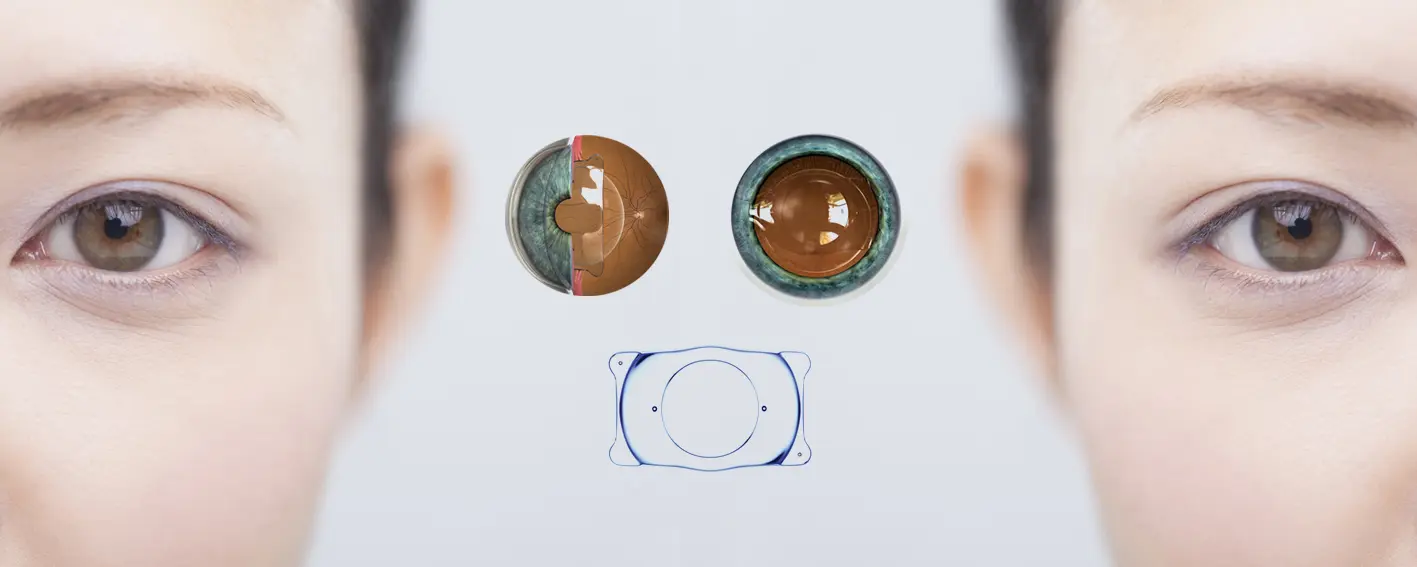
Phakic ICL surgery does not cause myopia recurrence
1. The Nature of “Regression”
“Regression” is usually understood as the return of myopia after treatment. In laser procedures, this occurs due to corneal structural changes over time.
With Phakic ICL, the situation is different. Since no corneal tissue is removed, the ICL lens remains fixed in place, keeping light refraction stable. Therefore, the risk of regression is nearly nonexistent. However, some factors still need consideration:
- Age-related refractive changes: Presbyopia or minor refractive shifts may occur with aging, requiring reading glasses.
- Development of other ocular diseases: Cataracts, glaucoma, or retinal disease may affect vision.
- Unstable prescription before surgery: If myopia was not stable for at least a year, refractive changes may still occur post-surgery.
2. Clinical Evidence
Reports from STAAR Surgical show that:
- 99.3% of patients achieved 20/40 vision or better within 6 months of surgery.
- 90% achieved 20/20 vision or visual acuity equivalent to their best corrected vision with glasses before surgery.
- Over 97% of patients expressed satisfaction and willingness to undergo the procedure again.
This demonstrates the long-term stability and reliability of Phakic ICL surgery.
3. Special Cases
Although regression does not occur in the traditional sense, there are situations where vision may change:
- Axial length elongation in younger patients with progressive myopia.
- Onset of other ocular conditions such as cataracts or glaucoma.
- Residual refractive error due to suboptimal surgical indication.
In such cases, ophthalmologists may:
- Replace the existing ICL lens with one of appropriate power.
- Or combine laser procedures (LASIK/SMILE) to correct residual refractive error.
Comparison Between Phakic ICL and Laser Refractive Surgery
| Criteria | Phakic ICL | LASIK/PRK/SMILE |
|---|---|---|
| Regression | Almost none | 5–10% after 5–10 years |
| Corneal impact | None | Yes (corneal ablation) |
| Dry eyes after surgery | Rare | Common |
| Suitable for high myopia | -3D to -20D, astigmatism 1–4D | Limited by corneal thickness |
| Reversibility | Yes (replaceable ICL lens) | Irreversible |
Expert Recommendations
- Undergo a comprehensive eye exam before surgery to check refractive stability, endothelial cell density, and anterior chamber depth.
- Attend regular post-op checkups to detect early complications such as elevated intraocular pressure or cataract formation.
- Maintain a healthy lifestyle: control blood sugar and blood pressure, and include eye-friendly nutrients (omega-3, lutein, vitamins A, C, E).
At TD Eye, patients receive personalized consultations, advanced diagnostic technology, and internationally standardized treatment protocols, ensuring the best long-term outcomes.
Conclusion
Phakic ICL surgery is a safe, sustainable, and nearly regression-free solution. Patients need not worry about corneal weakening or ectasia as with laser surgeries. Any changes in vision, if they occur, are usually due to natural biological factors or concurrent ocular conditions, which can be managed through routine follow-ups.
This method is safe, effective, and durable – particularly for patients with high myopia, thin corneas, or those concerned about dry eye complications from laser-based procedures.









 0916.741.763
0916.741.763 Appointment
Appointment