 vi
vi 23-Jan-2026
23-Jan-2026What Is Phakic ICL Surgery?

What are the conditions for Phakic ICL surgery?
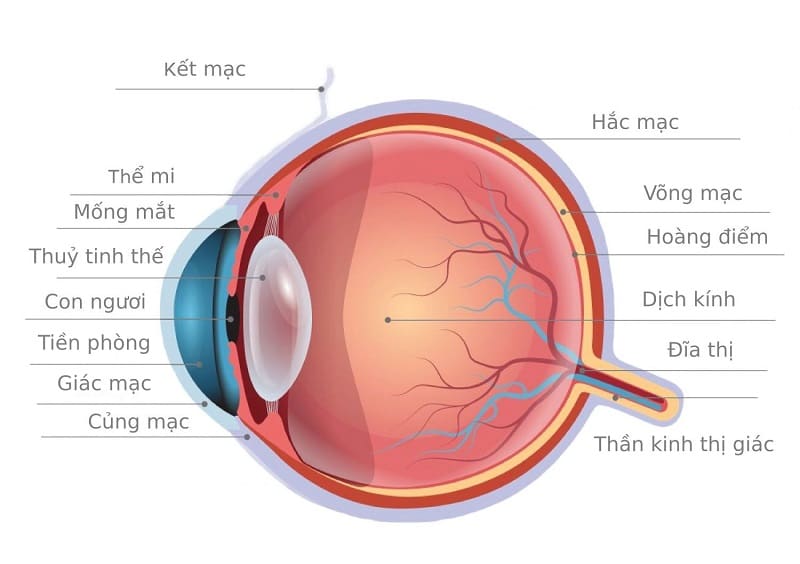
Phakic ICL is an intraocular lens implantation procedure in which the lens is placed behind the iris and in front of the natural crystalline lens, allowing refractive error correction without altering the corneal structure. Because this is an intraocular surgery, a comprehensive evaluation of both the anterior and posterior segments of the eye is required before surgery can be indicated.
Why Are People With High Myopia Interested in Phakic ICL?
In recent years, Phakic ICL has become a solution of interest for many patients with high myopia, particularly those who are not suitable candidates for LASIK or SMILE due to thin corneas or excessively high refractive errors.
However, this growing interest is often accompanied by very practical concerns:
- Can myopia greater than 9 diopters be corrected surgically?
- Is a corneal thickness of 520 µm safe?
- Is surgery advisable if retinal degeneration is present?
These concerns are entirely valid, and the answer cannot simply be “yes” or “no,” but rather must be based on a comprehensive set of specialized clinical parameters.
Mandatory Parameters to Measure Before Phakic ICL Surgery

Mandatory parameters before Phakic ICL surgery
1. Refractive Error (Myopia, Astigmatism)
Refractive error is always the first factor considered when evaluating a patient’s suitability for Phakic ICL surgery, as it forms the basis for determining whether this method can provide optimal visual correction. Phakic ICL is typically indicated for myopia ranging from approximately −3.0D to −20.0D, with or without associated astigmatism, depending on the selected lens type.
In clinical practice, for patients with high myopia exceeding 8–9 diopters, Phakic ICL is often regarded as a more appropriate option than laser-based procedures, as the lens is implanted inside the eye without ablating or further thinning the cornea. Therefore, cases of myopia greater than 9 diopters, such as the one mentioned, are usually considered for Phakic ICL from the outset rather than being excluded early, as many patients fear.
2. Corneal Thickness (CCT)
Corneal thickness is the factor that causes the most concern among patients, yet it is often misunderstood in the context of Phakic ICL. Many individuals have previously been advised that thin corneas preclude refractive surgery, leading to anxiety when they see a CCT measurement of approximately 520 micrometers. However, unlike LASIK or SMILE, Phakic ICL does not require corneal tissue ablation, meaning that thin corneas are not a primary exclusion criterion.
Nevertheless, corneal thickness still needs to be carefully measured and analyzed to assess overall corneal health and to rule out underlying conditions such as keratoconus or other structural abnormalities. In this context, a corneal thickness of around 520 µm is generally not considered a disadvantage for Phakic ICL, provided that all other ocular parameters meet safety requirements.
3. Anterior Chamber Depth (ACD)
Mandatory parameters before Phakic ICL surgery
Anterior chamber depth is one of the most critical and decisive parameters when considering Phakic ICL surgery. It represents the distance from the posterior surface of the cornea to the natural crystalline lens, which is precisely the space where the Phakic ICL will be implanted.
Typically, the anterior chamber depth must reach a minimum of approximately 2.8 mm, although the exact requirement may vary depending on the lens model and the surgeon’s assessment. When the anterior chamber is sufficiently deep, the lens can be positioned stably without obstructing aqueous humor circulation, thereby reducing the risk of elevated intraocular pressure or unintended contact with the crystalline lens.
In patients with high myopia, anterior chamber depth is often relatively favorable; however, precise measurement using specialized diagnostic equipment remains mandatory before a final surgical decision is made.
4. Corneal Endothelial Cell Density
Another important factor that is often overlooked by patients is corneal endothelial cell density. These cells are responsible for maintaining corneal transparency, yet they do not regenerate once lost. Prior to Phakic ICL surgery, the surgeon must ensure that the patient’s endothelial cell count remains above the age-adjusted safety threshold and shows no signs of abnormal decline.
This is because following intraocular surgery, endothelial cell density may gradually decrease over time. Therefore, assessing this parameter serves as a long-term preventive measure to protect visual quality not only immediately after surgery, but also for many years thereafter.
5. Retinal Condition
For patients with high myopia, retinal condition is always the most critical and sensitive factor requiring careful attention. High myopia leads to elongation of the eyeball, stretching the retina and increasing the likelihood of peripheral degenerative changes, as well as the risk of retinal tears or detachment. It is important to understand that Phakic ICL does not worsen retinal pathology; however, if pre-existing retinal lesions are present, a thorough fundus examination and advanced retinal imaging are mandatory.
In many cases, patients may require prophylactic retinal laser treatment prior to surgery to reinforce weakened areas, followed by a period of stabilization before lens implantation is considered. Therefore, retinal degeneration does not necessarily mean that Phakic ICL surgery is contraindicated, but rather that a more cautious and tightly controlled treatment pathway is required.
In cases combining myopia greater than 9 diopters, a corneal thickness of approximately 520 µm, and existing retinal degeneration, surgeons will not make hasty decisions. Instead, the evaluation process typically includes assessing refractive stability, measuring anterior chamber depth and corneal endothelial cell density, as well as performing meticulous fundus examinations and peripheral retinal imaging. If retinal lesions requiring intervention are detected, treatment will be carried out first, followed by a reassessment to determine whether Phakic ICL implantation is appropriate.










 0916.741.763
0916.741.763 Appointment
Appointment