 vi
vi 12-Jul-2025
12-Jul-2025Do myopia control glasses for children really work?

Children with myopia looking too closely – a common reason for early prescription of myopia control glasses.
School myopia – especially progressive myopia – is no longer a rare condition. WHO predicts that by 2050, about 50% of the global population will be myopic, with 10% developing high myopia (≥ -6.00D), leading to a higher risk of blindness due to retinal disease, macular degeneration, or retinal detachment. One proactive management strategy is the use of myopia control glasses. But the question remains: How effective are they, and what role does Phakic ICL play in future treatment?
1. What is progressive myopia and why control it early?
Progressive Myopia is diagnosed when the prescription increases by more than 0.5D/year. The core mechanism is axial elongation – not just refractive changes. This means that single-vision glasses only provide temporary clarity, but do not stop the underlying progression of disease.
Children with myopia >6.00D have a 44x higher risk of retinal detachment compared to non-myopic children.
2. Clinically proven myopia control methods
| Control Method | Main Mechanism | Effectiveness in Reducing Axial Elongation | Level of Evidence |
|---|---|---|---|
| DIMS lenses (Miyosmart) | Peripheral blur design → inhibits axial growth | ~59% | 2-year RCT (Lam et al., 2020, Br J Ophthalmol) |
| Stellest lenses (Essilor) | Microlens constellation → defocus control | ~67% | Essilor randomized trial, 2 years |
| Ortho-K (Orthokeratology) | Overnight corneal reshaping → peripheral optical modulation | ~40–60% | ATOM, ROMIO (IOVS) |
| Soft multifocal contact lenses (MFCLs) | Creates peripheral myopic defocus | 30–50% | BLINK Study (Ophthalmology, 2019) |
| Atropine 0.01–0.05% | Muscarinic blockade in retina and ciliary body | 50–60% | LAMP, ATOM 1–2 trials |
3. Scientific mechanism: Why do myopia control lenses work?
Animal models in mice and monkeys (form-deprivation myopia) show that lack of peripheral retinal focus signals axial elongation. Myopia control lenses like DIMS or Stellest are designed to send defocus cues to the retina that suppress excessive eye growth.
Human MRI scans show: each 1mm increase in axial length corresponds to ~2.5–3.0 diopters of myopia progression.
4. When to intervene, and with what method?

Intervention is recommended if:
- The child is <12 years old with myopia ≥ -0.50D
- There is a family history of high myopia
- Prescription increases >0.50D/year or axial length increases >0.1 mm/year
- Child has limited outdoor activity and high near work load
Recommended by group:
| Child Profile | Preferred Methods |
|---|---|
| Mild–moderate myopia, stable | DIMS, Stellest, Atropine 0.01% |
| Moderate–high myopia, fast progression | Ortho-K at night + DIMS during the day |
| Not suitable for contact lenses | DIMS or Stellest spectacle lenses |
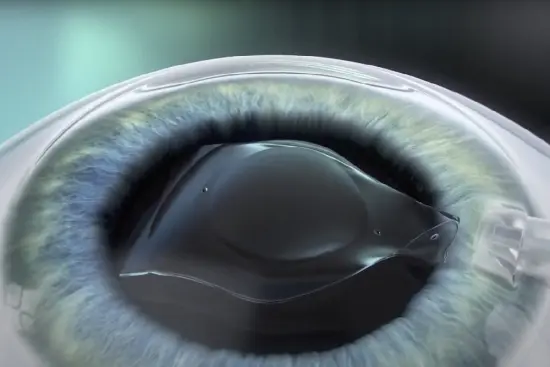
5. How is Phakic ICL related to myopia control?
Although Phakic ICL is not for children, it is a future treatment option for those who develop high myopia despite early interventions. Upon reaching age 21, Phakic ICL – a biocompatible lens that doesn’t affect corneal tissue – is ideal when:
- Myopia > -6.00D
- Cornea is too thin for LASIK
- Patient wants to stop using glasses without compromising eye health
Phakic ICL is FDA-approved to correct myopia from -3.00 to -20.00D and astigmatism from 1.00–4.00D, without inducing dry eye or damaging the cornea.
6. At TD Eye – We apply science to every child
At TD Eye, we measure axial length, corneal maps, and retinal OCT to customize plans based on real data:
- DIMS lenses for stable cases
- Ortho-K for moderate to high myopia
- Atropine for rapid progression
- Future Phakic ICL assessment for adulthood
Conclusion
Myopia control glasses are not just temporary aids – they are science-based strategies. Early intervention can prevent complications and prepare for safe refractive solutions like Phakic ICL.








 0916.741.763
0916.741.763 Appointment
Appointment